32-GPCR Safety Functional Assay Panel For Routine Off-Target Compound Profiling
Drug failures arising from safety-related concerns remain one of the biggest challenges facing researchers today (1). For any researcher or company, being able to profile putative lead compounds against established targets is vital to identifying a potential compound’s therapeutic efficacy and liabilities, including its on-target activity or off-target liability (2). G- protein coupled receptors (GPCRs) are amongst the most prominent drug targets in research today. They are known to play vital roles in central nervous system (CNS), cardiovascular (CV), pulmonary, and gastrointestinal (GI) conditions. While over 385 druggable GPCRs have been identified, many share similar affinities for the same ligands which can lead to lead compounds also interacting with more than one receptor.
Table 1: 32-GPCR Safety Targets in MULTISCREENTM Stable Cell Lines
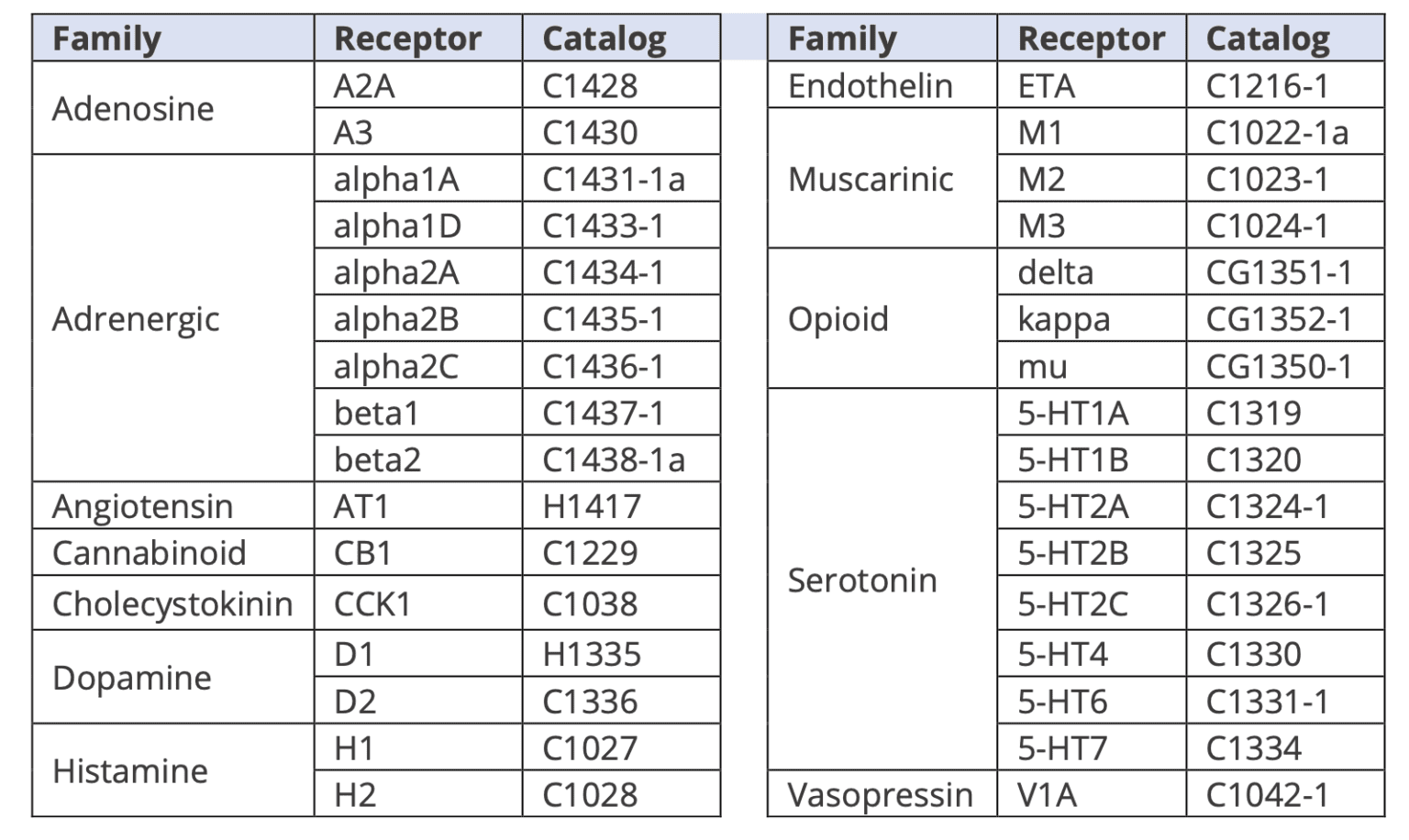
With Multispan’s Safety Functional Assay Panel (Table 1), compounds can be rapidly evaluated while accurately evaluating potential risks from off-target effects.
Why Profile GPCRs with Functional Assays vs. Binding Assays?
Using functional cellular assays, Multispan’s panel avoids the limitations of traditional binding assays for allosteric or non-functional binders, while also removing binding false positives. As a result, less time is wasted on investigating suboptimal leads, enabling you to select the best drug candidates to bring to market as quickly as possible.
MULTISCREENTM 32-GPCR Safety Functional Assay Panel
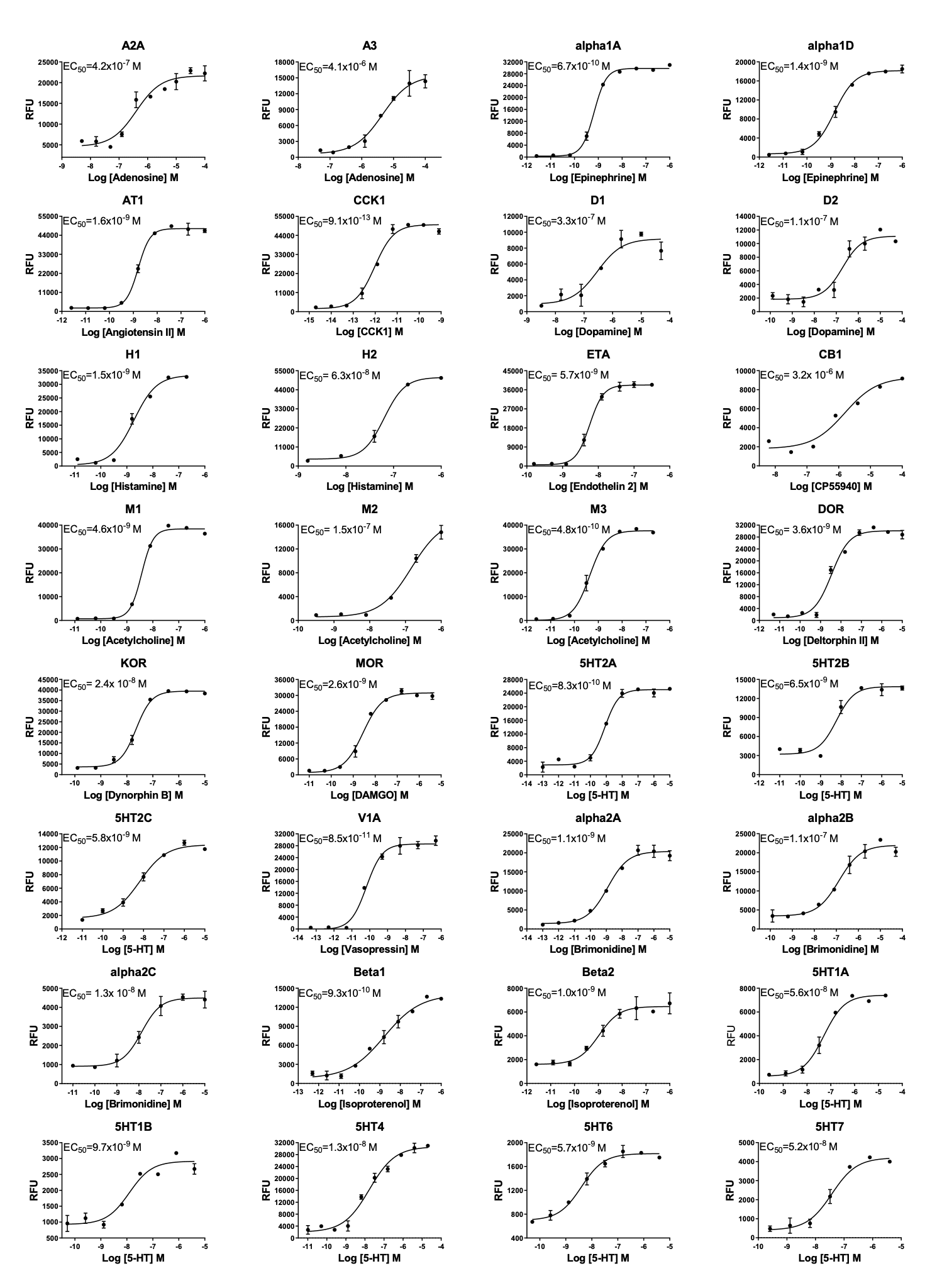
32 GPCR targets are included in the MULTISCREENTM 32-GPCR Safety Functional Assay Panel (Table 1). These GPCRS have been identified and reported in the literature by researchers and the pharmaceutical industry as important safety/liability targets. Specifically, the profile of each target family in the panel are summarized below and further detailed in Table 2.
Adenosine Receptors play important roles in regulating normal cell physiology while also acting as modulators in various disease processes. In the CNS, the receptors are involved in the release of neurotransmitters, synaptic plasticity and neuroprotection following ischemic insult, hypoxic, and oxidative stressors.
Adrenergic Receptors mediate the effects of a large array of clinically useful adrenergic drugs, including those that regulate blood pressure. Beta-adrenergic receptors are amongst the most well-studied of GPCR receptors with over 200 different types of receptors in the heart. Beta- receptors are amongst the most powerful regulators of cardiac function.
Angiotensin Receptors are known to regulate functions of the cardiovascular, hemodynamic, neurological, renal, and endothelial systems. As a result, they are important therapeutic targets for several diseases.
Cannabinoid Receptors are the most widely-expressed receptor protein from the GPCR family in the brain and are involved in various aspects of central neural activities and disorders, including appetite, learning and memory, neurodegeneration, epilepsy, stroke, anxiety, depression, multiple sclerosis, schizophrenia, and addiction.
Cholecystokinin Receptors bind the peptide hormones cholecystokinin (CCK) and gastrin. CCK1 receptors are found in the peripheral alimentary system and are involved in digestive tract- mediated satiety signalling, while CCK2 receptors are involved with memory, cognition, anti- analgesia, and anxiety.
Dopamine Receptors play roles in processes as diverse as motor control, information processing, neurological disorders, and addiction. Peripheral dopamine receptors mediate changes in blood flow via vasodilation, glomerular filtration rate, sodium excretion and catecholamine release.
Histamine Receptors (H1R–H4R) are characterized by their affinity for histamine. These receptors are known to play significant roles in the development of various allergic diseases, including asthma, allergic rhinitis, atopic dermatitis, and pruritus.
Endothelin Receptors bind endothelin produced by the vascular endothelium, with activation leading to increased smooth muscle contraction and potent vasoconstriction. Due to their potent vasoconstrictor properties, endothelin receptors have been implicated in the pathogenesis of hypertension, coronary vasospasm, and heart failure.
Muscarinic Receptors are the receptor sites for acetylcholine, the neurotransmitter of the parasympathetic autonomic nervous system. Five receptor types (M1-M5) are known. M1 receptors are located on autonomic ganglion, M2 on the ileum smooth muscle, vas deferens, and in the brain, and M3 in the smooth muscle of the GI tract, bladder, iris and endothelium.
Opioid Receptors have major subtypes m, d and k (mu, delta and kappa). They are present in numerous regions of the nervous system that are involved in pain transmission and control.
Serotonin Receptors play various roles in modulating the release of many hormones, including oxytocin, vasopressin, cortisol, prolactin, and substance P. Pharmaceutically, these receptors are amongst the most important and are the targets for antimigraine agents, antidepressants, antipsychotics, antiemetics, anorectics, and entactogens.
Vasopressin Receptors are comprised of the V1A, V1B, and V1C subtypes. The V1A types if localized to vascular smooth muscle, the myometrium, hepatocytes, brain cells, and platelets. V1A plays roles in vasoconstriction, myocardial hypertrophy, glycogenolysis, aggregation of platelets, and uterine contractions.
Table 2: Off-target Liabilities of the Selected 32 GPCR Targets
| Target | System | Activation or Agonism | Inhibition or Antagonism | Ref |
|---|---|---|---|---|
|
Adenosine A2A |
CNS, CVS |
Coronary vasodilation
↑ heart rate ↓ blood pressure ↓ platelet aggregation ↓ locomotor activity |
↑ blood pressure
↑ platelet aggregation ↑ tremor ↑ agitation ↑ insomnia ↑ arousal |
A |
|
Adrenergic alpha1A |
CNS, CVS, GI |
Smooth muscle contraction
↑ blood pressure Potential for heart arrhythmia ↓ insulin release |
↓ smooth muscle tone
↑ heart rate Potential for dizziness Impact on sexual function |
B |
|
Adrenergic alpha2A |
CNS, CVS |
↓ noradrenaline release
↓ sympathetic neurotransmission ↓ heart rate ↓ blood pressure |
↑ GI motility
↑ insulin release |
C |
|
Adrenergic beta1 |
CVS, GI |
↑ heart rate
↑ cardiac contractility ↑ renin release Relaxation of oesophagus and colon |
↓ heart rate
↓ blood pressure |
D |
|
Adrenergic beta2 |
CVS, Pulmonary |
↑ heart rate
↑ glycogenolysis ↑ glucagon release Peripheral vasodilation Potential for skeletal muscle tremor |
↓ blood pressure |
E |
|
Angiotensin AT1 |
CVS, CNS |
↑ vasoconstriction
↑ vasopressin release ↑ sodium retention ↑ sympathetic activity Suppression of renin secretion |
↓ vasoconstriction
↑ water retention Hypotension and dizziness Potential for hyperkalemia |
F |
|
Cannabinoid CB1 |
CNS |
↑ euphoria and dysphoria
↓ concentration Analgesia Potential for memory impairment/poor concentration Hypothermia |
↑ weight loss
emesis Potential for depression |
G |
|
Cholecystokinin CCK1 |
GI |
↑ gallbladder contraction; relaxation of the sphincter of Oddi
↑ bile to flow into the duodenum ↑ pancreas bicarbonate and fluid secretion from ductal cells ↑ exocrine pancreatic secretion ↓ gastric emptying ↑ relaxation of proximal stomach ↑ contraction of pylorus Potential for decrease symptoms of constipation predominant IBS and functional dyspepsia. |
↓ stimulation of pancreatic exocrine secretions
↑ gastric emptying of liquids ↑ development of gallstones |
H |
|
Dopamine D1 |
CNS, CVS |
↓ blood pressure; vascular relaxation ↑ dizziness; headaches ↑ nausea ↑ natriuresis Potential for abuse potential Potential therapeutic benefit in the treatment of Parkinson’s disease |
↑ mild to moderate, reversible depression
↑ anxiety; suicidal intent ↑ dyskinesia ↑ Parkinsonian symptoms (tremors) ↑ anti-emetic effects |
I |
|
Dopamine D2 |
CNS, CVS, endocrine |
↓ heart rate; syncope
↑ drowsiness Confusion; hallucinations ↑ sodium excretion; emesis ↓ pituitary hormone secretions |
↑ orthostatic hypotension
↑ drowsiness ↑ gastrointestinal motility |
J |
|
Endothelin ETA |
CVS |
↑ in blood pressure
↑ aldosterone secretion ↑ osteoblast proliferation |
Potential for teratogenicity |
K |
|
Histamine H1 |
CVS, Immune |
↓ blood pressure
↑ allergic responses; flush and wheal ↑ bronchoconstriction ↑ smooth muscle contraction ↑ capillary permeability |
↓ action of histamine
↓ in allergic responses ↑ sedation ↑ in body weight |
L |
|
Histamine H2 |
GI, CVS |
↑ gastric acid secretion
↑ positive inotropy Emesis |
↓ gastric acid secretion |
M |
|
Opioid (mu) |
CNS, CVS, GI |
Sedation; respiratory depression hypothermia ↓ gastrointestinal motility; Pupil constriction; Potential for abuse liability Miosis |
↑ gastrointestinal motility; dyspepsia; flatulence |
N |
|
Opioid (delta) |
CNS, CVS |
↑ analgesia; dysphoria
↓ respiration Psychomimetic effects Cardiovascular effects Modulation of hormone and neurotransmitter release |
↑ blood pressure
↑ cardiac contractility |
O |
|
Opioid (kappa) |
GI, CNS, CVS |
↓ colon transit time
↓ gastrointestinal motility ↑ urinary output sedation and dysphoria; confusion; dizziness ↓ locomotion tachycardia |
Insufficient information available |
P |
|
Serotonin 5HT1A |
CNS, endocrine |
↓ body temperature
↓ REM sleep ↑ ACTH; cortisol and growth hormone secretion |
Potentially anxiogenic |
Q |
|
Serotonin 5HT1B |
CNS, CVS |
↑ cranial vasoconstriction
↑ coronary artery vasoconstriction ↑ blood pressure ↓ release inflammatory neuropeptide |
↑ aggression |
R |
|
Serotonin 5HT2A |
CVS, CNS |
Smooth muscle contraction
↑ platelet aggregation Potential memory impairments hallucinations Schizophrenia Serotonin syndrome |
Insufficient information available |
S |
|
Serotonin 5HT2B |
CVS, pulmonary, development |
Pulmonary hypertension
Potential cardiac valvulopathy |
Possible cardiac effects |
T |
|
Vasopressin V1A |
Renal, CVS |
↑ water retention in body
↑ blood pressure ↓ heart rate ↑ myocardial fibrosis ↑ cardiac hypertrophy ↑ hyponatraemia |
Insufficient information available |
U |
|
A. Benarroch, E. E. Adenosine and its receptors: Multiple modulatory functions and potential therapeutic targets for neurologic disease. Neurology 70, 231–236 (2008).
B. Michelotti, G. A., Price, D. T. & Schwinn, D. A. α1-adrenergic receptor regulation: basic science and clinical implications. Pharmacol. Ther. 88, 281–309 (2000). C. Philipp, M., Brede, M. & Hein, L. Physiological significance of α2-adrenergic receptor subtype diversity: one receptor is not enough. Am. J. Physiol. Regul. Integr. Comp. Physiol. 283, R287–R295 (2002). D. Lohse, M. J., Engelhardt, S. & Eschenhagen, T. What is the role of β‐adrenergic signaling in heart failure? Circ. Res. 93, 896–906 (2003). E. Cazzola, M., Matera, M. G. & Donner, C. F. Inhaled β2-adrenoceptor agonists: cardiovascular safety in patients with obstructive lung disease. Drugs 65, 1595–1610 (2005). F. Michel Burnier Angiotensin II Type 1 Receptor Blockers. Circulation. 103:904–912 (2001). G. Le Foll, B., Gorelick, D. A. & Goldberg, S. R. The future of endocannabinoid-oriented clinical research after CB1 antagonists. Psychopharmacology (Berl.) 205, 171–174 (2009). H. Dufresne, M., Seva, C. & Fourmy, D. Cholecystokinin and gastrin receptors. Physiol. Rev. 86, 805–847 (2006). I. Peacock, L. & Gerlach, J. Aberrant behavioral effects of a dopamine D1 receptor antagonist and agonist in monkeys: evidence of uncharted dopamine D1 receptor actions. Biol. Psychiatry 50, 501–509 (2001). J. Emilien, G. et al. Dopamine receptors — physiological understanding to therapeutic intervention potential. Pharmacol. Ther. 84, 133–156 (1999). K. Palmer, M. J. Endothelin receptor antagonists: status and learning 20 years on. Prog. Med. Chem. 47, 203–237 (2009). L. Walsh, G. M. Emerging safety issues regarding longterm usage of H1 receptor antagonists. Expert Opin. Drug Saf. 1, 225–235 (2002). M. Hattori, Y. Cardiac histamine receptors: their pharmacological consequences and signal transduction pathways. Methods Find. Exp. Clin. Pharmacol. 21, 123–131 (1999). N. Trescot, A. M., Datta, S. & Lee, M. Opioid pharmacology. Pain Physician 11 (Suppl. 2), S133–S153 (2008). O. Barron, B. A. Cardiac opioids. Proc. Soc. Exp. Biol. Med. 224, 1–7 (2000). P. Walsh, S. L. et al. Enadoline, a selective κ opioid agonist: comparison with butorphanol and hydromorphone in humans. Psychopharmacology (Berl.) 157, 151–162 (2001). Q. Lacivita, E., Leopoldo, M., Berardi, F. & Perrone, R. 5‐HT1A receptor, an old target for new therapeutic agents. Curr. Top. Med. Chem. 8, 1024– 1034 (2008). R. Van de Kar, L. D. et al. ICV injection of the serotonin 5‐HT1B agonist CP‐93,129 increases the secretion of ACTH, prolactin, and renin and increases blood pressure by nonserotonergic mechanisms. Pharmacol. Biochem. Behav. 48, 429–436 (1994). S. Sun-Edelstein, C., Tepper, S. J. & Shapiro, R. E. Drug-induced serotonin syndrome: a review. Expert Opin. Drug Saf. 7, 587–596 (2008). T. Roth, B. L. Drugs and valvular heart disease. N. Engl. J. Med. 356, 6–9 (2007). U. Barrett, L. K., Singer, M. & Clapp, L. H. Vasopressin: mechanisms of action on the vasculature in health and in septic shock. Crit. Care Med. 35, 33–40 (2007). |
||||
How does it work?
With over 16 years of in vitro safety pharmacology experience, Multispan leads the way in providing researchers with the tools needed to help identify potentially unsafe compounds earlier in the drug discovery process.
Multispan’s panel has been specifically designed to assist researchers streamline the process of in vitro safety pharmacology profiling. To jump start your research, simply submit your compounds with instructions on handling, solubility, and storage. On the 1st workday of each month, Multispan’s expert teams runs the assay panel with your compounds (which can be submitted up to the last workday of the previous month). Multispan then profiles your compounds by FLIPR in Ca++ assays in agonist and antagonist modes, single point duplicates or 10-point duplicate dose-response curves according to your exact requirements. On the 4th workday of each month, analyzed and raw data is sent via email and uploaded into any specified database. To ensure your compounds are included in the Test Date of your choosing, submit your compounds and PO by the last working day of the month. Off-cycle timing and customized-panel profiling are available on demand.
Data Quality Assured In order to assure assay quality and consistency, 32 highly quality MULTISCREENTM stable cell lines (Table 1) are used. Each stable cell line clone has been rigorously selected, validated and QC’ed using the GPCR target’s endogenous ligand (Table 3)
Data quality from each compound profiling run is assured with:
- One control agonist run for each target.
- CV< 10% and EC50 value of the control compound DRC from run to run shall not exceed 101/2
- Any questionable data is repeated at no additional charge.
If you are generating new small molecules and biologics, and eager to identify their potential side-effects as potential therapeutics in “real-time”, Multispan can help!
References
(1) Kaczorowski GJ, Garcia ML, Bode J, Hess SD, Patel UA. The importance of being profiled: improving drug candidate safety and efficacy using ion channel profiling. Front Pharmacol. 2011;2:78. Published 2011 Dec 13. doi:10.3389/fphar.2011.00078
(2) Basith S, Cui M, Macalino SJY, Park J, Clavio NAB, Kang S and Choi S (2018) Exploring G Protein-Coupled Receptors (GPCRs) Ligand Space via Cheminformatics Approaches: Impact on Rational Drug Design. Front. Pharmacol. 9:128. doi: 10.3389/fphar.2018.00128
Table 3: Assay Performance 32-GPCR Safety Targets